
Medication Overuse Headache
Medication Overuse Headache
Medication Overuse Headache (MOH) is a syndrome related to the personal habit of overtreating headache with painkillers.
There is a great need for world wide education of the public about this problem.
This is an article by Britt Talley Daniel MD, retired member of the American Academy of Neurology, the American Headache Society, migraine textbook author, and blogger.
Medication overuse headache (MOH) used to be called Rebound Headache and in general is the occurrence of frequent or daily headaches which have Migraine features of being severe, throbbing, one-sided, nausea and vomiting, and sensitivity to sound and light. They are the most common cause of Chronic Migraine in the general population.
Related questions.
What is the Transformation of headache from episodic to chronic?
Chronic Migraine is a term used for a patient who has headache over 15 days a month, 8 of which have migraine features. A significant number of these patients have MOH which is now 80-90% of new patients seen in specialty headache clinics and affects 4 million people yearly.
Patients with chronic migraine due to overtreatment often can state the onset of their frequent headaches and the period of time they have had severe, chronic, near daily headaches. Patients may say 3 months, or 6 months, or a year, or the past 10 years, but others can’t answer this question.
When they had less than 15 headaches a month, they had episodic migraine, but when the headaches became more than 15 headache days a month or daily, then chronic migraine has developed. Overtreatment of headache is the basic reason for the transformation.
MOH occurs mainly with Migraine patients and sometimes with Tension Type Headaches. There is a transformation which occurs gradually over weeks to months. Many patients fluctuate in and out of Medication Overuse Headache depending on how bad their headaches are and how much medicine they take to treat it.
MOH is a concerning, disabling, well known, worldwide problem. It is the number 1 diagnosis for new patients to a headache practice and affects 1% to 2% of the general population. The problem with medication overuse headache is that patients typically rotate to different drugs and take many drugs at the same time that causes or worsens the headaches.
Many of these persons daily consume a lot of caffeine, often over 400 mg, which the Mayo Clinic states is the upper normal amount of caffeine per day. A key to their problem is that these patients often state they have to stay on daily caffeine and they get a bad headache if they try to stop.
Medication Overuse Headache comes from over treating with painkillers or headache medications such as simple over the counter drugs like caffeine, Tylenol or Advil, or more complicated drugs like opioid narcotics, pain killers with barbiturates, or triptans.
What drugs are usually taken that cause Medication Overuse Headache?
The International Classification of Headache Disorders (ICDH) 3 describes frequent headache from the following classes of drugs:
Non-opioid analgesic-overuse headache
Paracetamol (Tylenol, acetaminophen)-overuse headache
Non-steroidal anti-inflammatory drug (NSAID)-overuse headache
Acetylsalicylic acid-overuse headache
Combination-analgesic-overuse headache
Pseudoephedrine (Sudafed) the decongestant in over the counter sinus meds, such as Tylenol sinus or Advil sinus, or the D in Allegra-D
Tylenol (acetomeniphen)
Ergotamine drugs—Cafergot, Ergomar, Wigraine
Triptans--Imitrex (sumatriptan), Maxalt (rizatriptan), Zomig (zomatriptan, Axert (almotriptan), Relpax (eletriptan), Amerge (naratriptan), or Frova (frovatriptan)
Aspirin
Aspirin with caffeine—Excedrin, Anacin, NoDoz, Redline RTD
NSAIDS—(Nonsteroidal Anti-inflammatory Drugs) such as Motrin (ibuprofen, Advil), Naprosyn/Anaprox (Aleve), and Meloxicam
Narcotics—Vicodin (hydrocodone, Narco), Tramadol, Demerol, Nucynta, OxyContin, Tylenol with codeine
Drugs with barbiturates-- Fiorinal, Fioricet, Phrenilin, Esgic, generic butalbital.
How much medication does it take to cause MOH?
The International Classification of Headache Disorders 3 list of amounts of drugs taken which might cause medication overuse headache:
Triptans or Ergotamine intake >10 days/month (like sumatriptan)
Non-opioid simple analgesics >15days/month (aspirin, Tylenol, caffeine, or Advil)
Opioids or Analgesics combined with barbiturates >10days/month
What diagnoses do these patients think that they have?
56% of patients who have Migraine have never had a diagnosis by a doctor. These patients think they have Migraine aliases—Sinus headache, Menstrual headache, hungry headache, let-down headache, or nocturnal headache.
Patients with these features present to the doctor with Chronic Migraine due to Medication Overuse Headache.

Check out my Big Book on Migraine Here.
What are the clinical features of Medication Overuse Headache?
There are two clinical features to this syndrome:
Daily or very frequent headaches which are one-sided, throbbing, and associated with sensitivity to light and sound, nausea, vomiting, and irritability,
This syndrome causes serotonin, a calming brain neurochemical, levels to drop so the patient may also develop or worsen preexisting anxiety, depression, poor concentration, panic attacks, and insomnia, which also are core symptoms of the disorder.
Migraine is comorbid (means they occur together) with Depression 50%. Generalized Anxiety Disorder and Panic Disorder 40%.
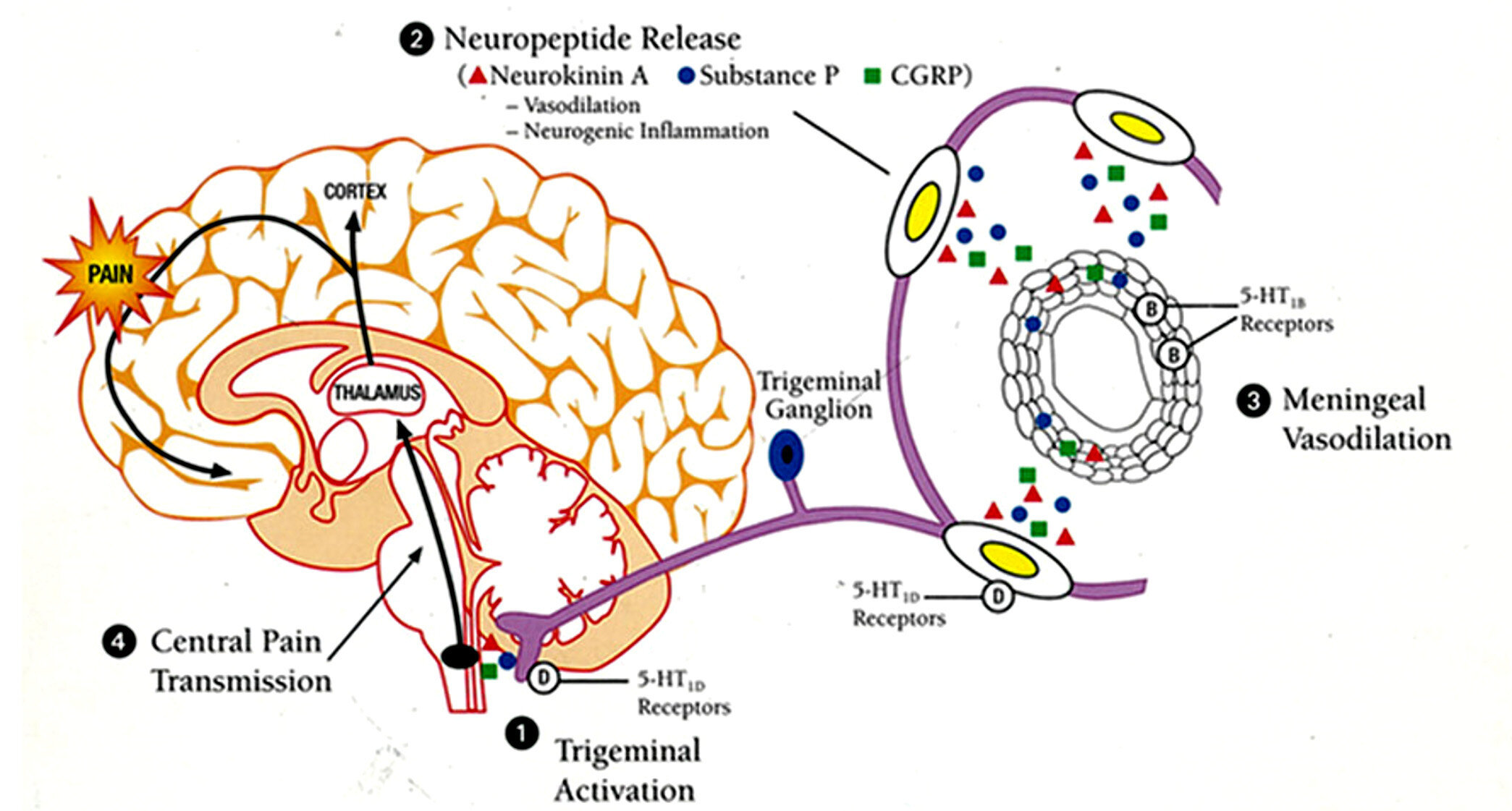
The Migraine timing cycle
The migraine timing cycle. There are 4 steps in the migraine process which I like to call the migraine timing cycle.
The first step is trigeminal inflammation by the brainstem.
Then the second step at 20-40 minutes the ganglion of the nerve and artery in the brain start to release the Neuropeptides: Neurokinin A, Substance P, and CGRP.
Then at about 2 hours the release of these chemicals causes the 3rd step which is meningeal artery vasodilatation.
The 4th step at 3-4 hours since onset is inflammation of the thalamus, a deep nucleus in the center of the brain which is called the “pain center” of the brain.
The 4th step is also called “Central Sensitization” because steps 1,2, and 3 occur in the skull but are outside the brain (trigeminal nerve, nerve and arterial ganglions, cerebral arteries.) Step 4 inflames the thalamus, a deep nucleus inside the brain.
Why does transformation occur?
A single episode of migraine may last from 4-72 hours. That is, a migraine may last up to 3 days. Patients may tell me that their migraines sometimes last a week, or 5 days and that is not a single episode of migraine, but most likely chronic migraine, which usually comes from overtreating.
What is going on here? It is from metabolic features in the brain related to the release of the inflammatory, vasodilating neurochemicals—Substance P, Neurokinin, and CGRP.
If the patient keeps taking medication through the entire length of their 3 day migraine it comes about so that after 3 days pass every time they take a cup of coffee (home-130 mg of caffeine), Tylenol, Sumatriptan, or at worse hydrocodone, or Tramadol, or at the very worse—a headache barbiturate drug such as Fiorinal, they get three more days of the bothersome neurochemicals and the headache just keeps going on.
When the brain becomes sensitized to these drugs repeat dosing causes neuro-inflammatory chemicals to be released in the brain which keeps the headache going.
I saw a migraine patient once who was 64 when we met and she had been overtreating with Advil since her mother told her it was okay to take it, using 4-10 every day since she was 6 years old.
I saw another man who was 60 who had been taking up to 10 Excedrin migraine tablets (each with 65 mg of caffeine) a day since he was a child.
They both improved by detoxing off the medications they had been taking.
And these are benign stories mixed in with countless patients who come in taking hydrocodone or Tramadol, both of which are opioid narcotics.
The Worst acute migraine drug is clearly a drug with a barbiturate in it, such as Fiorinal. Marilyn Monroe overdosed on a barbiturate drug and died. Barbiturate drugs stay in the body for a long time and don’t dialyze out with overdose, a fact, plus the headache problem which has limited their use although where I practice in Dallas, Texas non-neurologist doctors use a lot of it and were probably advised to give Fiorinal in medical school.
Barbiturate headache drugs have been banned in every country in the world except Canada and the United States because they are notorious for causing Medication Overuse Headache.
The sad statement heard at Headache meetings in the US is that “Barbiturate headache drugs are the only reason to go from Mexico to the US for purchase.” Apparently, you can buy hydrocodone in Mexico without a prescription, but you can’t buy Fiorinal.

In bed with a severe Migraine

Treatment of Medication Overuse Headache
The best treatment for medication overuse headache is stopping the offending drugs, usually on 1 day, or sometimes by tapering over several weeks if the patient has been on a high dose of an opioid or barbiturate for a long time.
The patient needs to be on a Migraine preventive drug, preferably one of the new CGRP drugs, do the Migraine lifestyle, and limit acute therapy to no more than 2 days a week.
In the US sometimes we just want to take a “pill” and have whatever medical problem we have go away, to disappear. Going away won’t happen with headache if the patient keeps treating.
Consider my Mini eBook on Migraine Here.
This site is owned and operated by Internet School LLC, a limited liability company headquartered in Dallas, Texas, USA. Internet School LLC is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Although this site provides information about various medical conditions, the reader is directed to his own treating physician for medical treatment.
All the best.
Follow me at: www.doctormigraine.com, Pinterest, Amazon books, and YouTube.
Britt Talley Daniel MD